Dr. Pieter-Jan Vandekerckhove, Belgium: Advancing robotic knee surgery program beyond the learning curve from 5 to 7 procedures per day
At AZ Sint-Jan Brugge, robotic-assisted knee surgery is no longer new. The initial phase of adoption, including the learning curve and achieving time neutrality, has already been completed. The workflow is established, the team is aligned, and the system works.
But for Dr. Pieter-Jan Vandekerckhove, that was not the endpoint. It was the starting point for the next question:
How do you add more cases to the same 9-hour OR day without asking more from the team?
Moving beyond time neutrality
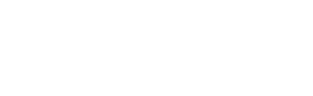
Early implementation confirmed that robotic-assisted knee surgery could be performed without increasing operative time. The team reached the same stable throughput as with conventional surgery, with five procedures per operating room day, supported by a standardized and repeatable workflow.
Rather than maintaining that level, Dr. Vandekerckhove focused on refinement by understanding each individual process step and reducing variation across the entire system.
Through detailed, data-driven analysis of workflows, roles, and timing, small inefficiencies were identified and addressed. Transitions became smoother. The rhythm of the operating day became more predictable.
The result was a gradual but meaningful improvement in performance.
Within the same 9-hour operating room slot, the team progressed from five procedures per day in February 2025 to six by November 2025. By March 2026, they were increasingly performing seven robotic-assisted knee surgeries.
Optimization as a continuous process
What distinguishes this phase is the level of detail. Optimization was no longer about major structural changes, but about fine-tuning:
Aligning anesthesia, preparation, and surgical timing
Standardizing roles and responsibilities within the team
Reducing unnecessary variation in instrumentation and setup
Creating consistent turnover patterns between cases
Parallelization of tasks during preparation and breakdown
Digital twin analysis confirmed that performance at this level is not driven by speed alone, but by system-wide alignment. That alignment is what makes it possible to increase volume without increasing pressure on the team.
Each small improvement contributed to a more stable and predictable workflow, and that predictability enabled scale.
Higher surgical case volume often comes at a cost: higher stress, greater workload, or reduced team satisfaction. What is notable here is that this increase did not rely on pushing the team harder. It relied on building a system that supports the team.
Standardization reduced uncertainty. Predictability reduced cognitive load. Optimized instrumentation reduced physical strain, translating into measurable ergonomic benefits, including reduced lifting and improved posture during key surgical steps.
At higher volumes, these factors become even more important.
A practical and scalable way of working
Dr. Vandekerckhove describes this approach as both practical and scalable: Achievable not just in theory, but sustainable in daily practice for both him and his team.
The experience at AZ Sint-Jan Brugge illustrates a different phase of robotic surgery adoption: not implementation, not validation, but maturation.
A phase where data replaces assumption, consistency replaces variation, and incremental improvements enable meaningful scale.
It demonstrates that robotic-assisted knee surgery is not only about introducing new technology, but about continuously improving the system around it. This is what ultimately allows programs to scale with confidence.